
Experienced Attorneys Protecting the Rights of the Neglected and Abused
The Nursing Home Law Center is committed to providing the legal resources necessary to hold negligent facilities accountable.

In the early stages, bed sores often look like a discolored or tender area of skin over a pressure point, while later stages can look like a blister, an open wound, a crater, or a deep ulcer with visible tissue. Bed sore pictures can be difficult to look at, but they often help families recognize when a skin change may be the start of a serious pressure injury.
Speaking with a bedsore lawyer from our firm after any suspicious decline in a nursing facility can help families understand what happened, preserve key evidence, and assess whether the resident received appropriate care.
In this guide, we explain what bed sores look like at each stage, where they usually appear, and what families should watch for when a loved one is in a nursing home.
This article discusses and describes wounds that may be upsetting to view in real-life photos.
Real photos of pressure ulcers help, but we caution families against self-diagnosis based solely on images. Lighting, ointment, and skin color can change how a wound appears. The Johns Hopkins pressure injury guide and the Cleveland Clinic bed sores guide both stress that these wounds worsen quickly when pressure remains in place.
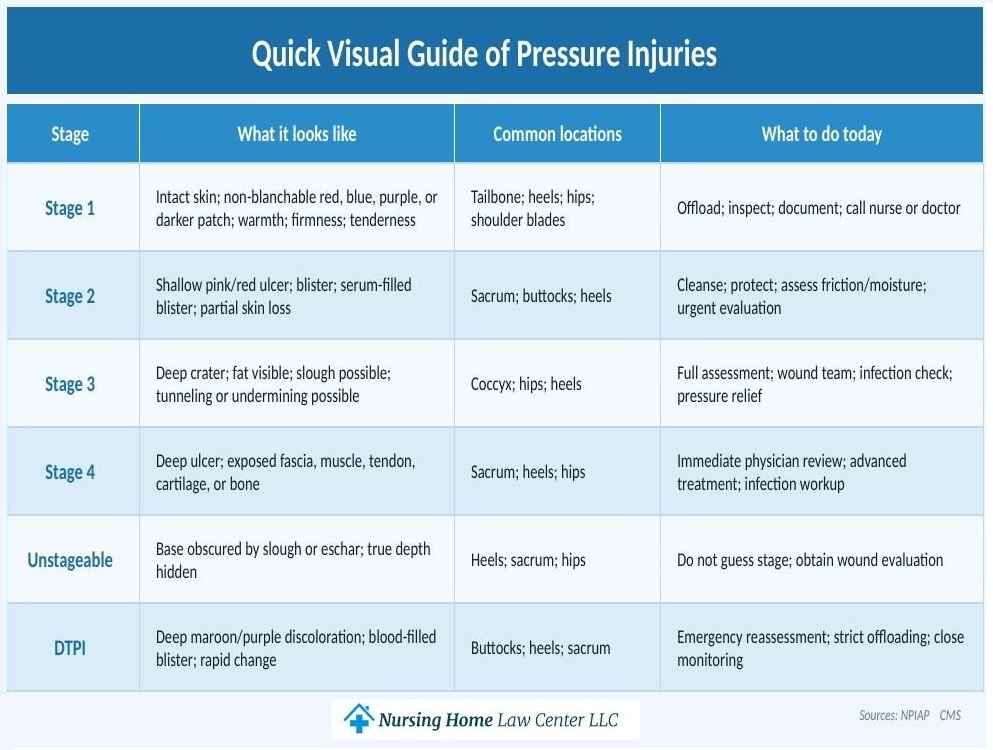
Below, we explain how these wounds typically appear in stages 1 through 4, as well as unstageable ulcers and deep tissue pressure injuries.
Call (800) 926-7565 Toll-Free for a No Obligation Consultation
In stage 1, the skin is still intact. On lighter complexions, the affected area often appears red or pink and does not blanch when pressed. Skinsight’s guide points out that on darker complexions, the change may look blue, purple, maroon, ashen, warmer, firmer, or simply different from nearby healthy skin.
Common misreads include ordinary blanchable redness after brief pressure, an incontinence rash, or a temporary crease mark. Experts emphasize non-blanchable change of intact skin, sometimes with altered sensation or temperature, before a visible break appears. Families comparing stage 1 bed sore photos should still ask a healthcare provider to confirm what they are seeing.

In stage 2, the blood flow is compromised, and there is partial-thickness loss with exposure of the dermis. A stage 2 bed sore may appear as a shallow pink or red ulcer or a serum-filled blister. The wound bed is usually moist and viable, without slough or thick eschar.
Common misreads include skin tears, tape injuries, fungal rash, or moisture injury from incontinence.


A stage 3 ulcer shows full-thickness tissue loss of the skin. Fat may be visible, the sore often looks cratered, and the wound extends into deeper tissue. Families may see a hollow with irregular edges, drainage, odor, or yellow slough.
Common misreads include assuming black or yellow material is always “healing scab” when it may actually be dead tissue. A stage 3 bed sore can develop into a tunneling bed sore, and untreated depth increases the risk of bed sore infections, surrounding skin infections, bone infections, and joint infections.


In stage 4, the wound reaches the deepest category in the ordinary staging system, with exposed or directly palpable fascia, muscle, tendon, cartilage, or bone. These are severe sores.
Common misreads include thinking the dark or yellow skin covering is the entire injury when the actual cavity extends further. This level can become life-threatening, especially if the infection spreads. Families reviewing a stage 4 bed sore should know that advanced ulcers can lead to osteomyelitis, sepsis, and, in the worst cases, bed sore fatalities.


The depth of an unstageable bed sore cannot be confirmed because slough or eschar blocks the view. That means the base is covered, and clinicians cannot see how far tissue loss goes until the covering is appropriately addressed.
Common misreads include calling it “just a black scab” or assigning it a stage based on a photograph. WebMD notes that once slough or eschar is removed, a deeper wound, such as stage 3 or stage 4, may be revealed, though stable heel eschar is a separate judgment call.


DTPI often appears as a deep red, maroon, or purple area or as a blood-filled blister. The top layer may still be intact even while deeper tissues have been severely injured.Common misreads include calling it a simple bruise. These injuries can evolve rapidly and may look different on dark skin tones. A broader overview of the stages of bed sore development can help place DTPI beside the other categories.


Call (800) 926-7565 Toll-Free for a No Obligation Consultation
When we review cases from nursing homes, we focus first on the same-day response. Staff should relieve pressure on the wound site, reassess turning schedules, document the wound’s size and appearance, and initiate appropriate wound care.
If your loved one is on bed rest, has a spinal cord injury, or lacks enough upper body strength for independent repositioning, the prevention plan should be even tighter because those are major risk factors. The MSKTC guide to recognizing and treating pressure sores is useful for families dealing with limited mobility after spinal cord trauma.
We also look for daily prevention basics: changing positions to ease pressure, keeping the skin clean and dry, using skin-care products such as moisture-barrier creams, and closely monitoring nutrition and hydration.
Cleveland Clinic advises repositioning every 15 minutes in a chair or every 1 to 2 hours in bed when possible, while Mayo Clinic advises prompt evaluation if the area fails to improve within 24 to 48 hours, and urgent review if the area develops fever, drainage, foul odor, warmth, or swelling. Those are classic signs of infection. The facility’s compliance with CMS pressure ulcer guidelines often becomes central when we assess neglect.
Call (800) 926-7565 Toll-Free for a No Obligation Consultation
They usually appear where skin lies over bone with little padding. Common sites where pressure sores develop include the tailbone, hips, heels, ankles, elbows, spine, shoulder blades, and other bony areas.
The biggest risk factors and the most common causes of bed sores are limited mobility, friction, shear, moisture, reduced sensation, incontinence, poor nutrition, fragile skin, and illnesses that impair circulation. People on bed rest and people with spinal cord injury are at especially high risk.
Yes. Some pressure sores form quickly, and authoritative sources note that they may arise over hours or days, or even within a few hours without movement. That is why families should act as soon as they notice signs, rather than waiting a few weeks for them to resolve. Knowing how fast bed sores develop is essential if a facility claims the wound appeared overnight due to reasons beyond its control.
Several conditions can look similar at first glance. A diabetic ulcer may appear on the foot because of neuropathy and circulation issues rather than sustained pressure. A Kennedy terminal ulcer can emerge near the end of life and raises a different clinical discussion. Moisture rash, bruising, skin tears, and friction injuries can also cause confusion, especially in darker skin tones, where color changes are less obvious.
No. Some residents are medically complex, and some wounds occur despite good care. But nursing home residents should still receive a risk assessment using the Braden Scale, receive assistance with turning, receive nutrition support, have prompt documentation, and receive a plan to prevent pressure injuries. Whether families can sue a nursing home for bed sores often turns on who was liable for bed sores, what the chart showed, and whether the proper protocol was actually followed.
Potentially, yes. We look at whether staff cleaned the wound, protected the surrounding skin, managed moisture, ordered appropriate pressure wound treatment, and escalated when signs of infection appeared.
Deep wounds may require bed sore debridement to remove dead tissue, as well as specialized dressings or products such as DuoDerm. Depending on the depth and extent of the infection, doctors may use antibiotics, surgery, or skin grafts to close the wound and promote healing. Families should not assume petroleum jelly alone is adequate wound treatment.

At our firm, we look closely at photo progression, charting gaps, turning logs, nutrition records, and whether the facility acted quickly enough to reduce pressure, fight infection, support wound healing, and protect healthy skin before a small injury became a severe sore that families find online. Chronic nonhealing wounds can also create rare long-term complications, including squamous cell carcinoma.
A nursing home abuse and neglect lawyer can review whether staff failed to relieve pressure, keep the affected area clean, or obtain timely physician care after visible pressure injuries appeared. We also examine whether the wound was allowed to deepen from stage 1 to stage 2, then to stage 3 or stage 4, whether staff documented the wound bed correctly, and whether treatment was aimed at skin healing rather than papering over decline.We handle these cases on a contingency fee basis, which means you pay no lawyer fees unless we win your case. We encourage families to review prior bed sore settlements when weighing next steps. If you want our team to assess photos, records, and the care timeline, contact us today for a free consultation.

Nursing home abuse lawsuits must be pursued according to the laws set forth by the state where the facility is located. In this section, our attorneys have compiled the relevant laws, regulations and local organizations for each state so you can get an idea of how the law impacts your situation. Should you decide to move forward with a case, you will also find information about locating an experienced attorney who can assist your family.